





Dentistry in the Horse

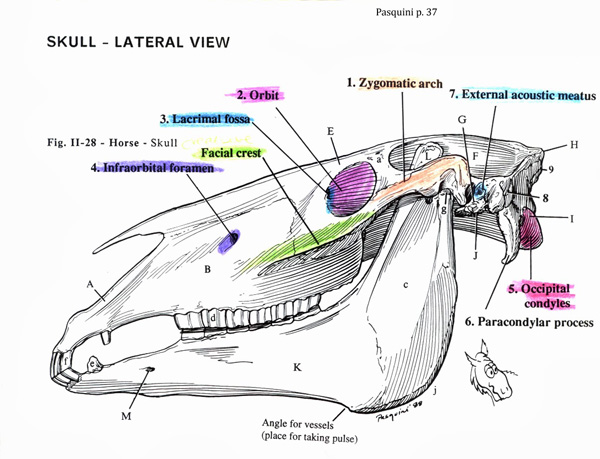
Image courtesy Fox Run Equine Center
By Brian S. Burks, DVM, Diplomate, ABVP, Board Certified Equine Specialist
You would not have your oral cavity and teeth examined by an unlicensed individual, nor would you take your dog and cat to anyone but a veterinarian. Rather, you would seek out someone who received undergraduate education, followed by professional medical education. Your horse also deserves to have the oral cavity evaluated by a veterinarian who is trained in anatomy, physiology, pharmacology over eight years of education rather than a two week course, or worse, picking up tools with zero education. Equine dentistry is much more than simply filing sharp points on molars and premolars.
The goal of equine dentistry is to keep the masticatory unit of the horse functional. In adult horses, this requires dental work at least annually, but the higher the performance level, the more often dental examination should be performed. Small dental problems can affect not only mastication, but the horse’s response to the rider. Dentistry should remove sources of oral discomfort. These include sharp enamel points, wolf teeth, and long, sharp canine teeth, along with a myriad of other problems.
Dental disorders can cause a variety of behavioral abnormalities, including:
• Head tossing
• Bit chewing
• Refusal to carry the bit
• Frequently trying to open the mouth
• Reluctance to take a certain lead
• Reluctance to bend the poll or neck
• Running backwards
• Wide turns
• Not stopping squarely
• Rearing
• Unexplained temper fits
Oral pain may cause a horse to eat slowly or incompletely, dunking hay in the water bucket before eating, have cheek swelling that comes and goes, and may have difficulty maintaining weight in the face of increased rations. Horses with dental problems may not perform to their fullest potential; timed events off by even a second can be the difference between winning and losing.
During dental examination, the external structures of the head should be evaluated first. Any abnormal swelling or draining tracts are noted. Facial asymmetry may be evident; the ears may not be as mobile as normal, there may be drooping lips, and the eyes may have lid abnormalities or not be level.
The mandible has a normal lateral excursion, usually only a few millimeters, and the cheek teeth should come into contact during this excursion. The jaw should move freely, and if not, this may be a sign of overgrown teeth.
Once the horse is sedated, and a speculum is in place, the soft tissues inside the mouth should be examined for trauma, infection, or tumors. Sometimes the mucosa will be calloused, indicating long-term exposure to sharp enamel points. Any malodorous breath should be noted; if present, evaluation for a tooth root infection is needed, which will need to be corrected surgically.
Fractured teeth should be noted and radiographed; most will need to be removed. Horses can get dental caries, or demineralization of the teeth. They are brown or black areas in the cementum. Diastemata are also important to note; these gaps between the teeth cause food trapping with subsequent rotting and bacterial colonization of the gingiva. These gaps may be due to missing teeth, abnormally positioned teeth, or angulation of the most caudal or cranial teeth causing compression on the other teeth.
Hooks and ramps are common abnormalities that interfere with mastication and affect comfort of the horse. They can sometimes block the side-to-side movement of the jaw and put pressure on the temporomandibular joint. The horse may resist collection because the head carriage required increases pressure on the over-long teeth and the TMJ. Rostral maxillary hooks can pinch the cheek mucosa when pressure is put upon the bit. Hooks require reduction, but if they are too long, care must be taken not to enter the pulp cavity. Waiting several months prior to complete reduction allows dentin formation to protect the pulp.
A wave mouth is an undulating occlusal surface, involving multiple teeth. It can become quite pronounced, causing significant oral dysfunction, and should be dealt with early by flattening the occlusal table; in severe cases it is not possible to completely correct the undulation. In some cases, it may be easier to palpate, rather than see the wave. The most common presentation is for the first one to three mandibular cheek teeth to be long, with the corresponding maxillary teeth being too short.
The cause of wave mouth is unclear, but several factors may affect the conformation of the teeth:
• Different rates of eruption may occur due to asynchronous shedding of deciduous teeth.
• Periodontal disease may delay tooth eruption
• Dental caries may cause increased wear.
• Mechanical forces exerted on static maxillary teeth by mobile mandibular teeth, creating tooth loss.
Treatment is by slowly flattening the occlusal surfaces over 1-2 years. Some cases are impossible to correct completely. Overzealous correction may leave spaces between the arcade occlusal surfaces, leading to the inability to grind food.
Step mouth is due to a missing tooth, leading to over-eruption of the now unopposed tooth. This leads to the tooth growing into the empty socket, damaging the gingiva and to the inability for the jaw to move properly. The teeth may drift toward the center of the gap, leaving diastema, rostrally or caudally, to form. This condition occurs secondary to trauma or to tooth root infection and subsequent extraction. This condition needs to be treated every six months, to keep the tooth short enough not to cause problems.
Shear mouth is an arcade with an angled occlusal surface greater than 15 degrees. The cheek side of the maxillary teeth is quite long, while the lingual side is quite short, even to the gingival surface. The mandibular teeth are a mirror image. The condition may affect one or both sides of the mouth. One sided shear mouth may be due to displacement of the hemi-mandible.
The incisor teeth may develop ventral (smile) or dorsal curvature (frown). The former is associated with increased angulation of the incisor teeth. It may impair lateral excursion and should be at least partially corrected. Dorsal curvature is associated with cribbing. An irregularly uneven incisor surface is called a step bite and is often secondary to trauma. The tooth may become fractured or undergo a tooth root infection, resulting in loss of the tooth.
There are many dental abnormalities that may occur in the horse. Treatments have improved, but some disorders remain difficult or impossible to repair completely. Prevention by regular dental care is a must.
foxrunequine.com